Booking a slot online for your Covid-19 vaccination means you are presented with a screen asking ‘Do you know your NHS number?’ If you do, then you can use it to book a date and time for your jab. It is remarkable that the NHS has been in existence for more than 70 years and yet we can use it without needing to know our NHS number or being required to show it when we access healthcare services. This article explains the history of this important number.
How do people in England & Wales get an NHS number?
In 1996, everyone registered with an English or Welsh GP was allocated a new NHS number. People in Scotland already had a CHI (Community Health Index) number, and there is a separate arrangement for Northern Ireland where health and social services are run by the same authority).
But I don’t remember being issued with a new NHS number in 1996?
That’s because while a new central database was created, the new numbers were not sent out to the public or to patients. The new numbers were used first by GPs and then gradually by hospitals and community health services.
What about babies born since 1996?
There is a mechanism that allows hospital staff to use their maternity computer system to obtain an NHS number for a new-born baby from the national system. This number is then shared with the local child health services computer system. These systems are used to provide health visitors with details of new-born babies and to manage the immunisation and vaccination of babies and children.
Why was there a need to issue a ‘new’ NHS number?
When the NHS was established in 1948, it started to use the national identity number that had been issued to everyone in September 1939 at the start of the World War 2. But this use was restricted to just the administration of GP services, including the payment of GPs; hospitals continued to use their own pre-NHS patient numbering systems. Overtime, with just manual processes in use, some people managed to get more than one NHS number, and some managed to get the same number as someone else. By 1996, there were about 17 different formats in use, so the government agreed that a new NHS number should be issued, to facilitate the increasing use of computer systems within the NHS and the need for these systems to be able to exchange information between different healthcare providers (for example, GPs and hospitals) about patients. For more historical details see the appendix at the end of this article.
What does the ‘new’ NHS number look like?
All NHS numbers are 10 digits long, and are of the format 123 456 7890, and when displayed on screen and on paper they are supposed to be shown in this ‘3-3-4’ format.
What does the term ‘valid’ mean in the context of an NHS number?
The tenth digit is a ‘check digit’, to help the person entering the NHS number to make sure they have not mis-typed any digits. By the time the user has typed in the first 9 digits an algorithm built into the computer system has already worked out what the tenth digit should be; if the user gets any of the digits wrong then the number will not be accepted as ‘valid’.
So, a ‘valid’ NHS number is one that exists, or could exist?
Yes, ‘valid’ does not mean that it is the right number for a particular patient.
Does the possession of an NHS number mean that you are eligible for free NHS care?
No. It is possible to be allocated an NHS number, but not be entitled to free NHS care. And the reverse is true: for example, a resident of Scotland who has emergency treatment in an English hospital is entitled to free NHS care, even though they do not have an NHS number because they are not registered with an English GP practice.
Why can’t hospitals allocate NHS numbers to patients like the Scottish resident in the above example?
Patient identification is not always straightforward – not everyone keeps the same name throughout their life and consistently uses the same name in all encounters with all government agencies or always carries identification, and patients are not required to present their NHS numbers when receiving treatment. It would not make sense to ask busy A&E receptionists delay a patient’s treatment while they try to find a patient’s NHS number on the national database and, if necessary, to allocate a new number to the patient in front of them. The national database of NHS numbers would soon get ‘corrupted’ with duplicates. Hence hospitals continue to use their own numbering systems (usually called casenote numbers or medical record numbers) in their Patient Administration Systems (PAS), and to allocate new numbers from these systems to new patients (like the emergency Scottish patient). In practice, and to minimise risks to patient safety caused by misidentification or using incomplete patient records, hospitals use their own numbering systems alongside the NHS number (when they know it).
If a hospital doesn’t allocate new NHS numbers, then how does it obtain the NHS number for a patient whose details are not already known to its Patient Administration System?
The trusts that run hospitals each have an important back-office function to manage this task. Typically, every day the trust sends off to the central database a data file of new PAS registrations; within a few hours the file is returned with verified NHS numbers now included alongside names, where this has been possible. The proper name for the central database is the Personal Demographics Service (PDS), the national electronic database of NHS patient details such as name, address, date of birth and NHS number.
So, an NHS number is classed as ‘verified’ when it has been confirmed that it does indeed relate to the specific patient?
Yes, note the difference between ‘valid’ and ‘verified’.
So, it’s a simple process?
Not always. The hospital’s back-office staff are required to work on the returned data file to sort out any anomalies (for example, because of name changes). It is of critical importance that the right NHS number is attached to the patient’s hospital computer record.
So, it’s not always straightforward, and the NHS number is important?
Correct. Once you have obtained your NHS number, keep it with you always. In an emergency, the possession of your NHS number may be critical in enabling a health care provider to identify your records easily and hence deliver treatment with the full knowledge of your medical history. A number which started life as an essential tool of war-time government and then became a means of ensuring GPs were paid appropriately is now an essential tool for the safe treatment of patients, including ensuring the smooth running of the Covid-19 vaccination programme.
Appendix
The origin of the original NHS number, what it was used for and why it had to be replaced.
In 1938, as war seemed inevitable, plans were accelerated to enable a comprehensive national registration scheme to be available the following year. Lessons were learnt from the First World War when, in 1915, there had been a National Registration scheme for persons aged 15-65; owing to the lower age limit, it would not have been able to fulfil its main purpose of recruiting for national service had the war not ended in 1918.
World War 2 broke out on 3 September 1939, and less than a month later, on the night of Friday September 29th, each householder completed a return of everyone spending the night in that household. On or after Saturday September 30th, 65,000 enumerators went out to collect the completed returns and issue identity cards. Official information encouraged completion by pointing out that a full return was in the public’s interest, since the information collected would be used to allocate food and clothes rations. (It would also be used to check up on men who had failed to register for military service.)
An example of the front cover and inside pages of an identity card is shown below:
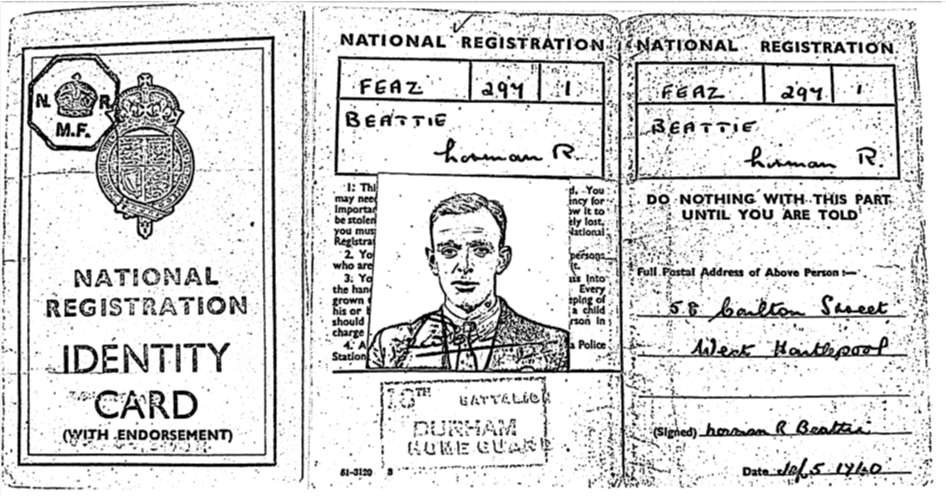
The National Registration identity number (which became his NHS number) is written twice: FEAZ2971. People born before 1996 may remember having an NHS number of a similar format.
Below is an extract from the 1939 register, showing what was recorded for each resident.

(second from the bottom).
Some records include names crossed out with another name written in an annotation above or at the side, signifying the tracking of the population over time (during and after the war) with the addition of women’s married names and other name changes. The management of the central register was the responsibility of a Civil Service department that had been relocated to a hotel in Southport (the Smedley Hydro) requisitioned by the government at the start of the war. (The North West coast of England was an ideal spot for relocation, due to its rail network, distance from Europe – and German bombers – and the large number of premises available for requisition.)
National Registration was abolished in February 1952, and the Minister of Health announced that the Government had decided that it was no longer necessary to require the public to possess and produce an identity card or to notify change of address for National Registration purposes, though the numbers would continue to be used in connection with the National Health Service.The national registration records had been used to prepare the National Health Service Central Register (NHSCR) ready for the first day of the NHS on 5th July 1948, and so even though National Registration ended in 1952 the civil servants in Southport remained in place to run the NHSCR.
For those people who held identity cards, the number on the card became their NHS number. Babies were issued with NHS numbers at the time of birth registration and immigrants and anyone whose original number could not be traced were allocated numbers on a different system as the need arose. The NHSCR was therefore a register of NHS patients which was kept up to date from returns sent by the local registrars of births and deaths and family practitioner committees (FPCs). The NHSCR data was needed to work out how many NHS patients were registered with each GP so the government knew how much to pay the GP for providing NHS services. Transfers of patients between FPCs were recorded as a by-product of a patient leaving a GP in one area of the country and registering with a different GP near to their new place or residence. The task of handling all these movements of patients and relying on paper returns from GP practices and local registrars helps to explain why the NHSCR became inflated and inaccurate, and why ‘new’ NHS numbers eventually had to be issued.
(Sources: Nissel M, People Count: a history of the General Register Office, 1987; Central Register anniversary publication, Southport 1999.)
The views and opinions expressed are personal and are not necessarily those of Northumbria Healthcare NHS FT.
Posted April 2021
